The Metabo-oncology Company
Metabo-oncology — the overlap of obesity + cancer — is the next wave in cancer patient treatment.
Cancer cells co-opt metabolic hormones (e.g., insulin, leptin) to proliferate, resulting in cancer progression and metastases. Yet, the many cancer patients also have insulin resistance. This metabolic state affects millions of cancer patients worldwide is overlooked as a major contributor to cancer progression. What’s worse, many anti-cancer treatments cause metabolic dysfunction, limiting treatment effectiveness and even leading to treatment resistance.
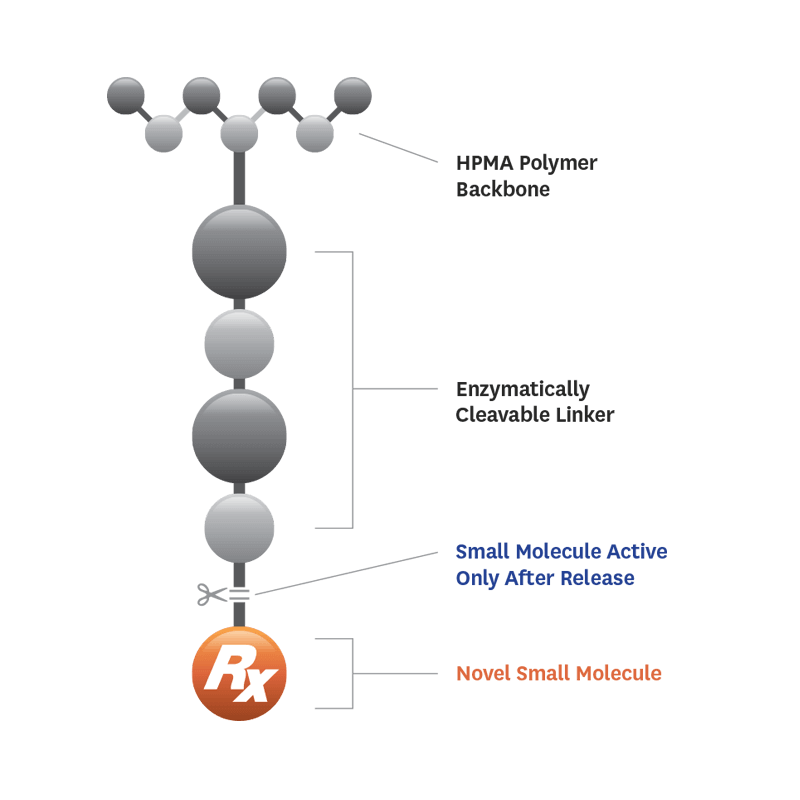
SynDevRx – the leader in the emerging field of metabo-oncology – is tackling this urgent and unmet medical need with its clinical drug evexomostat (SDX-7320).

-
Treating Cancer and Metabolic Hormone Dysfunction
It’s a fact: People with systemic metabolic hormone dysfunction, which is common in obese and overweight individuals or people with excess belly fat, type 2 diabetes or pre-diabetes, are more likely to get — and die from — cancer. In 14% of men and 20% of women (U.S.), deaths by cancer are directly related to dysregulated metabolic hormones.
Among the most commonly dysregulated metabolic hormones are insulin, leptin and adiponectin, each of which contribute to tumor growth and metastases (insulin, leptin) or suppress tumor growth (adiponectin). Treating metabolic dysfunction in cancer patients is critical for standard-of-care therapies to work to their full potential.
No novel therapy is available for the hundreds of thousands of patients suffering from this silent killer.
SynDevRx has the first clinical drug candidate – evexomostat/SDX-7320 – specifically targeting this unmet medical need.
-
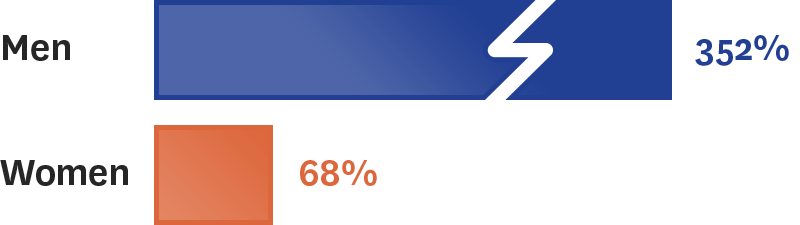
Liver Cancer
Men with a body mass index (BMI) between 35 and 39.9 were found to have a 4.52-fold (i.e. 352%) increase in the relative risk of death from liver cancer (Calle et al, 2003, New Eng J Med, 348(17):1625-38). In the same study, women with a body mass index (BMI) between 35 and 39.9 were found to have a 1.68-fold (i.e. 68%) increase in the relative risk of death from liver cancer.
Increased risk of death from cancer when obese:
-
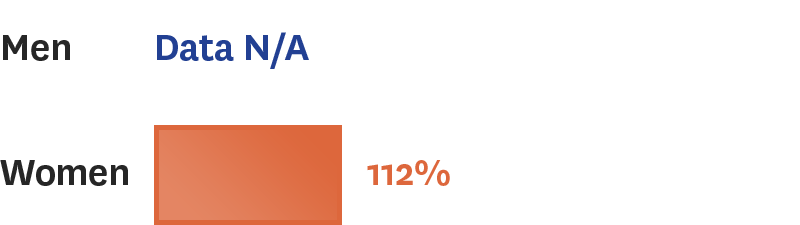
Breast Cancer
Post-menopausal women with a body mass index (BMI) between 30 and 34.9 were found to have a 1.6-fold (i.e. 60%) increase in the relative risk of death from breast cancer (Calle et al, 2003, New Eng J Med, 348(17):1625-38). In the same study, women with a body mass index (BMI) between 35 and 39.9 were found to have a 1.7-fold (i.e. 70%) increase in the relative risk of death from breast cancer, and women with a BMI ≥ 40 had a 2.1-fold (i.e. 112%) increase in the relative risk of death from breast cancer.
Increased risk of death from cancer when obese:
-
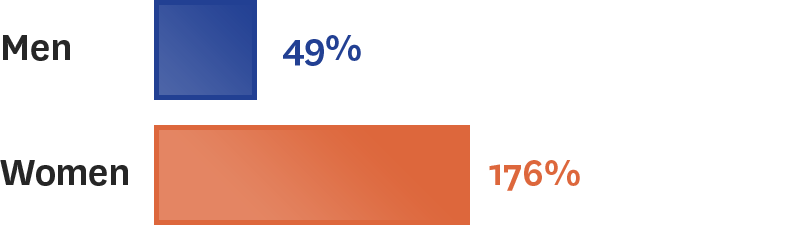
Pancreatic Cancer
Men with a body mass index (BMI) between 35 and 39.9 were found to have a 1.49-fold (i.e. 49%) increase in the relative risk of death from pancreatic cancer (Calle et al, 2003, New Eng J Med, 348(17):1625-38). In the same study, women with a body mass index (BMI) between 35 and 39.9 were found to have a 1.41-fold (i.e. 41%) increase in the relative risk of death from pancreatic cancer, while women with a BMI ≥ 40 had a 2.76-fold (i.e. 176%) increase in the relative risk of death from pancreatic cancer.
Increased risk of death from cancer when obese:
-
Uterine (endometrial) Cancer
Women with a body mass index (BMI) between 30 and 34.9 were found to have a 2.53-fold (i.e. 153%) increase in the relative risk of death from uterine/endometrial cancer (Calle et al, New Eng J Med; 2003, 348(17):1625-38). In the same study, women with a body mass index (BMI) between 35 and 39.9 were found to have a 2.77-fold (i.e. 177%) increase in the relative risk of death from uterine/endometrial cancer, while women with a BMI ≥ 40 had a 6.25-fold (i.e. 525%) increase in the relative risk of death from uterine/endometrial cancer.
Increased risk of death from cancer when obese:

-
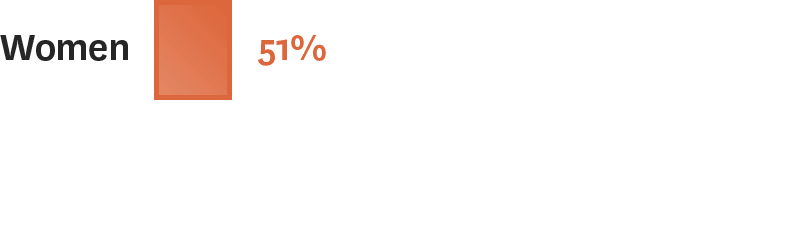
Ovarian Cancer
Women with a body mass index (BMI) between 30 and 34.9 were found to have a 1.16-fold (i.e. 16%) increase in the relative risk of death from ovarian cancer (Calle et al, New Eng J Med; 2003, 348(17):1625-38). In the same study, women with a body mass index (BMI) between 35 and 39.9 were found to have a 1.51-fold (i.e. 51%) increase in the relative risk of death from ovarian cancer. A more recent meta-analysis of nine studies found that women who were obese (BMI ≥ 30) had a 1.17-fold (i.e. 17%) increase in risk of dying from ovarian cancer (Nagle et al, British J Cancer, 2015; 113:817–26.
Increased risk of death from cancer when obese:
-
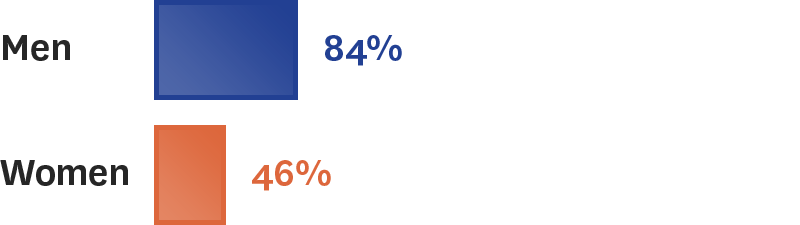
Colorectal Cancer
Men with a body mass index (BMI) between 35 and 39.9 were found to have a 1.84-fold (i.e. 84%) increase in the relative risk of death from colorectal cancer while women with a body mass index (BMI) between ≥ 40 were found to have a 1.46-fold (i.e. 46%) increase in the relative risk of death from colorectal cancer (Calle et al, New Eng J Med; 2003, 348(17):1625-38).
Increased risk of death from cancer when obese:
-
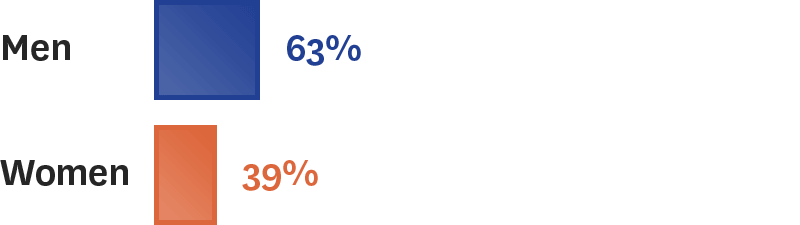
Esophageal Cancer
Men with a body mass index (BMI) between 30 and 34.9 were found to have a 1.28-fold (i.e. 28%) increase in the relative risk of death from esophageal cancer while men with a body mass index (BMI) between 35 and 39.9 were found to have a 1.63-fold (i.e. 63%) increase in the relative risk of death from esophageal cancer (Calle et al, New Eng J Med; 2003, 348(17):1625-38). In this study there was no statistically significant increase in the relative risk of death from esophageal cancer in women with increased BMI.
Increased risk of death from cancer when obese: